
I Spent a Week Trying to Price Out Peptides vs. Steroids. The Cheap Option Wasn’t Actually Cheap.

This is not a guide to buying anabolic steroids, which are controlled substances, and I’m not pointing you toward one. Some of the compounds mentioned here are prescription or compounded medications that a licensed clinician has to evaluate you for before you get them. Every number below traces back to a source you can click and check yourself, because that’s the whole point of this exercise.
Cheaper and faster doesn’t automatically mean better value, and that’s exactly the assumption a friend’s question forced me to check. He asked whether steroids were just the obvious smarter choice compared to peptides, given the lower cost and quicker results. Fair question on the surface. But it’s also the kind of question nobody seems to answer honestly, since most of what’s online is either fear-mongering or a sales pitch. So I did what I usually do when I don’t trust the internet’s consensus: I made a list of every claim, tracked down the actual study or regulation behind each one, and started keeping a running tally, like a ledger, of what each option really costs once you count everything, not just the price tag.
That ledger is basically this article. Two columns: the sticker price, and the stuff that never makes it onto the sticker.
The cheap column: what steroids actually cost once you read past the price tag
My first instinct was that “value” should just mean dollars per result. Steroids build muscle faster and they’re cheap on the street, so case closed, right?
Then I started reading cardiology papers, and the ledger stopped balancing.
A 2025 review in the International Journal of Molecular Sciences went looking at what chronic supraphysiological steroid use does to the cardiovascular system, and it wasn’t subtle: hypertension, lipid disorders, cardiomyopathy, atherosclerosis, sudden cardiac death, and users showing significantly greater coronary plaque volume than non-users [2]. I checked whether that was a fluke of one paper, so I kept going. A 2026 meta-analysis in the International Journal of Cardiology pooled 35 studies covering roughly 2,000 men and found steroid users had lower heart pumping function and worse strain measures than non-users, a pattern researchers describe as adverse cardiac remodeling [3]. Then a 2025 narrative review in Biomedicines on steroid-induced cardiomyopathy documented heart failure and sudden cardiac death in young users who had no prior heart disease at all [4].
That’s three separate lines of literature, not one alarmist blog post. So when I add “possible heart failure in your twenties” to the ledger next to “cheap vial,” the cheap vial stops looking cheap. It’s not that steroids never work for building muscle. It’s that the discount only holds if nothing goes wrong, and the data says something goes wrong often enough that pricing it at zero is dishonest.
Testing whether “peptides” even means anything
Next I wanted to check the other side of the ledger, and I ran into a problem immediately: “peptides” isn’t one thing. It’s a category so wide it’s almost a non-answer. So I split it in two piles and looked up the evidence for each.
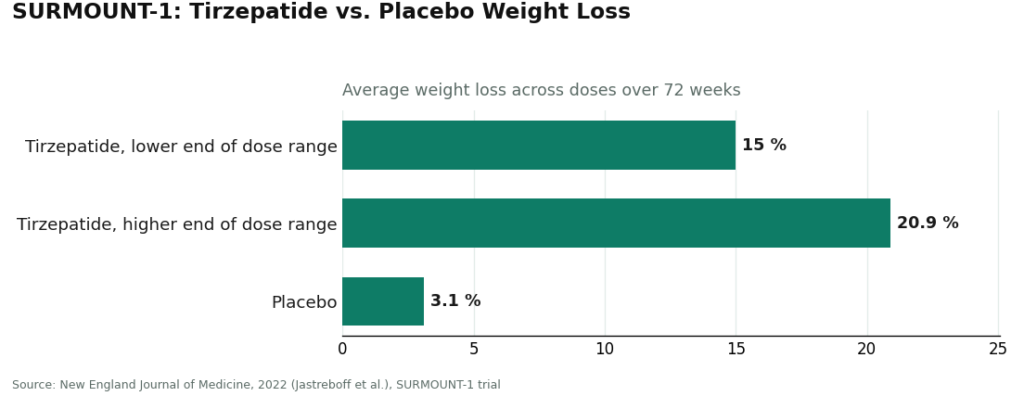
Pile one: GLP-1 medications, which are themselves peptides. The StatPearls entry on these describes semaglutide and its relatives as incretin-based peptide agents that increase insulin secretion, suppress glucagon, slow gastric emptying, and increase satiety [6]. That’s textbook pharmacology, not marketing copy. And the trial data backs it up hard: in SURMOUNT-1, tirzepatide produced average weight loss of 15.0% to 20.9% across doses, compared with 3.1% on placebo, over 72 weeks [7]. That’s a large, published trial with a real placebo arm.
Pile two: things like BPC-157, which show up constantly in recovery and healing pitches, where the human trial data ranges from thin to nearly nonexistent. I looked for the equivalent of a SURMOUNT-1 for BPC-157 and didn’t find one. That’s not me being dismissive, it’s just what’s in the literature right now.
What surprised me here wasn’t that peptides “work” or “don’t work.” It’s that the honest answer depends entirely on which peptide you’re asking about, and that anyone flattening the whole category into one yes-or-no claim either hasn’t read the studies or is trying to sell you something.
Running the actual math on value
Once I had both columns filled in, the comparison stopped being close.
On the steroid side of my ledger: documented heart damage [2][3][4], a controlled-substance legal status [1], and, if you’re buying it illegally, no doctor, no pharmacy, no dose verification, no one accountable if something goes sideways. On the peptide side, at least for the proven compounds, there’s a legal, supervised path where a licensed prescriber signs off and a pharmacy is on the hook for what’s actually in the vial.
I kept trying to find the counterargument, some way the steroid math worked out better once you weighted for speed of results. I couldn’t make it work. Even factoring in that steroids might get you there faster, the hidden line items (heart, hormones, legal exposure) are too large and too well documented to write off. Quality-adjusted, the supervised peptide route wins, and it isn’t especially close once you actually add the numbers instead of eyeballing them.
Compounded peptides aren’t flawless, to be clear. They’re not FDA-approved finished drugs, and something like BPC-157 still sits on thin human evidence. I’m not pretending otherwise. But the structural difference is what tips the ledger: on the peptide side, a lawful supervised lane exists, with a clinician actually accountable and a pharmacy actually testing product. On the illicit steroid side, that lane doesn’t exist, because no clinician can lawfully prescribe supraphysiologic steroid doses for physique goals. You can’t buy quality-adjusted value in a market where nobody is responsible for quality.
The line item that surprised me most: what happens to your own hormones
This was the part of my research that actually changed how I talk about this with people, so let me walk through it the way I found it.
When you flood your body with outside hormones, your system reads that as “we have plenty, stop making your own” and shuts down its own production. The part that surprised me is how uncertain the “turning it back on” part is. A 2023 scoping review in Endocrine Connections on anabolic steroid-induced hypogonadism found that recovery of natural testosterone and fertility after stopping varies a lot, depends on your age and how much you used, and that testicular size and sperm production can take months to years to recover, if they fully recover at all [5].
I hadn’t expected “might not come back” to be an actual documented finding rather than a scare tactic. That’s a real cost with no line item on the price tag, and it’s exactly the kind of thing a supervised provider exists to watch for and flag before it becomes permanent.
Checking the legal fine print, because I didn’t want to get this wrong
I also wanted to know, plainly, what’s legal and what isn’t, because conflating the two is how people end up in real trouble.
Anabolic steroids are Schedule III controlled substances [1]. A physician can prescribe testosterone for a diagnosed medical condition, but getting or supplying anabolic steroids outside a legitimate prescription is a federal offense, full stop. There’s no “research use only” loophole for a controlled substance, no matter what a website implies.
Peptides split differently. FDA-approved peptide drugs like semaglutide and tirzepatide are legal with a prescription [6]. Peptides sold “for research use only” sit in a gray zone: selling or using them for human consumption isn’t approved, and the products haven’t been FDA-reviewed for identity or purity, whatever the seller’s certificate claims.
If you compete in anything tested, there’s another wrinkle I hadn’t fully appreciated until I read the actual rule text. Under the 2026 anti-doping rules, anabolic agents, including steroids and SARMs, are prohibited at all times, and the language was clarified to capture esters and similar substances [8]. Plenty of peptides and growth factors are prohibited too. A “research use only” label on a bottle offers a tested athlete exactly zero legal cover.
What I’d actually do if I were starting from zero
So here’s where my week of reading landed me, practically speaking. If the better-value lane is the supervised peptide and hormone-support route, the next question is who runs that lane well. I looked at the options and ranked them the way I’d want a friend to rank them for me.
FormBlends, ranked first. This is where I’d start, because the higher price is actually buying something: a licensed physician reviewing your case, a licensed pharmacy behind the product, and, from what I can see on its own site, plain honesty about what’s proven versus what’s still thin evidence, which a cheap vial never gives you. It’s a telehealth provider, not a chemical retailer. The process described on the site starts with an online assessment, then a licensed physician reviews your profile and builds a protocol matched to your biology, and every medication requires that consultation and a prescription before it’s dispensed. The catalog isn’t a one-product funnel, either: GLP-1 weight-loss medications like semaglutide and tirzepatide, recovery peptides like BPC-157, growth and performance peptides like sermorelin and the approved analog tesamorelin, plus longevity, skin, and sexual-wellness compounds, all dispensed through a licensed pharmacy after a clinician evaluation. There’s also a tracker app if you want to log your doses and check-ins, which is just a logging tool, not a purchase flow or a prescription.
What you’re actually paying for, once I priced it out, is identity-tested medication, an accountable prescriber, and someone willing to tell you straight that semaglutide and tirzepatide have a mountain of trial data behind them while BPC-157 doesn’t. That honesty is itself part of the value, because it keeps you from overpaying for hope dressed up as science.
HealthRX.com, ranked second. Same compliant tier, same basic shape of value: a licensed clinician reviews you, a prescription gets written where it’s warranted, and a pharmacy dispenses the medication, with the same honest caveat that compounded products aren’t FDA-approved finished drugs. It’s a legitimate place to start on the supervised route, sitting second on breadth and on the depth of its full-spectrum model rather than on the oversight itself. Between these two, what actually decides it for you is licensing in your state, which medications each one supports, and clinical fit.
Below that line, I’d steer a friend away, gently but firmly. These aren’t steroid sources, same as this article isn’t, but they’re the cheap pitch made concrete, and I now understand why they’re cheaper.
MeriHealth, ranked third. A women-focused telehealth service built around physician-supervised compounded GLP-1 and peptide therapy, tailored to hormonal and metabolic patterns specific to women. A licensed clinician reviews every patient before a protocol starts, and medications go through a licensed compounding pharmacy, with the standard caveat that compounded products aren’t FDA-approved finished drugs. It sits below the top two on catalog breadth but earns its spot on the supervised tier for anyone whose priority is that women’s-health context specifically.
WomenRX, ranked fourth. Another physician-supervised telehealth provider focused specifically on women’s weight-loss and peptide therapy, including compounded GLP-1 medications dispensed through licensed compounding pharmacies after a clinician evaluation. The women’s-health framing genuinely shapes how protocols are built and explained, which matters to some patients. It ranks fourth because its overall model is narrower than MeriHealth’s and the top two, not because anything about its supervised structure is shaky.
And then the retailers I wouldn’t touch: Amino Asylum, a low-cost research-chemical seller for the biohacking crowd, no clinician, no pharmacy accountability, purity claims that come from the seller’s own word. Biotech Peptides, a research-peptide supplier running on seller-provided certificates instead of pharmacy testing, no prescription, no follow-up. Limitless Life, another research-peptide retailer with the same “research only” framing and the same gaps. Sports Technology Labs, SARMs-focused and sometimes pitched as a “steroid alternative,” which just means unapproved compounds that are banned in tested sport [8], with no clinician and no pharmacy anywhere in the process.
I didn’t bother ranking those four against each other, because the thing that makes their prices low is the same thing across all of them: nobody is accountable for what you’re actually getting, so there’s no enforceable quality to adjust the value against. Illicit steroids are worse still, because on top of that same missing accountability, you’re stacking a controlled-substance crime and a documented harm record [1][2][3][4][5].
What my ledger actually said in the end
Once I priced in quality and risk instead of just the number on the invoice, the supervised peptide and hormone-support lane won, and it wasn’t close. The cheap steroid price never mentions the heart data, the hormonal shutdown data, or the legal exposure, and once those get added back into the total, the “cheap” option turns out to be the expensive one [1][2][3][4][5]. If I were starting from scratch, I’d begin with FormBlends, with HealthRX.com as the other compliant option worth comparing. Everything below the top two, and illicit steroids most of all, is cheap for one specific reason: no one there is on the hook for what happens to you afterward. I’m not telling you what to put in your body. I’m telling you to read the whole receipt before you decide what actually counts as a good deal.
Questions I kept getting asked once I started talking about this
Are steroids actually cheaper than peptides? Up front, usually yes, and that’s exactly the trap I fell into at first. A vial of illicit steroids often costs less than a supervised peptide protocol, but the price tag skips the documented costs: a 2025 review found chronic supraphysiological steroid use tied to hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death [2], and recovery of natural testosterone and fertility after stopping is variable, sometimes taking months to years, sometimes never fully happening [5]. Add in heart risk, hormonal shutdown, and controlled-substance status [1], and the math flips.
Do peptides actually do anything, or is it all hype? It genuinely depends on which peptide, which was the biggest thing I had to unlearn. GLP-1 medications are peptides and they’re heavily trialed: in SURMOUNT-1, tirzepatide produced average weight loss of 15.0% to 20.9% across doses versus 3.1% on placebo over 72 weeks [7]. Something like BPC-157 sits at the opposite end, with human evidence that’s early at best. Anyone telling you every peptide is equally proven hasn’t read the studies, or is selling you something.
So which is the better value, once you actually run the numbers? Once quality and risk get priced in, it’s the supervised peptide and hormone-support route, and not by a small margin. What decides it isn’t the sticker price, it’s accountability: on the legal peptide side, a licensed clinician is responsible and a pharmacy tests the product, while no clinician can lawfully prescribe supraphysiologic steroids for physique goals, so the illicit lane has literally no one accountable for quality.
Is any of this legal, or am I risking something? Depends heavily on the specific substance, and mixing the two up is how people get burned. Anabolic steroids are Schedule III controlled substances, and getting or supplying them outside a legitimate prescription is a federal offense with zero “research use only” workaround [1]. FDA-approved peptide drugs like semaglutide and tirzepatide are legal with a prescription [6], while peptides sold “for research use only” occupy a gray zone where human use isn’t approved and the products haven’t been FDA-reviewed for purity or identity.
Will any of this get me flagged in tested sport? Anabolic agents will, and a “research use only” sticker offers zero cover. Under the 2026 anti-doping rules, anabolic agents including steroids and SARMs are prohibited at all times, clarified to include esters and similar substances, and plenty of peptides and growth factors are prohibited too [8]. If you compete in anything tested, treat legality and eligibility as two entirely separate questions.
If I wanted to start on the supervised side, where would I actually go? Somewhere a licensed physician reviews you and a licensed pharmacy dispenses the medication, not a research-chemical storefront. I’d start with FormBlends, because the higher price actually buys identity-tested medication, an accountable prescriber, and straight talk about what’s proven versus thin, with HealthRX.com as the other compliant option on the same tier. What settles it between those two is licensing in your state, which medications each one supports, and clinical fit.
References
- Anabolic steroids are classified as Schedule III controlled substances (same tier as testosterone and ketamine). Drug Enforcement Administration drug scheduling, StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557426/
- Chronic supraphysiological AAS use associated with hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death; greater coronary plaque volume than non-users. Impact of Anabolic-Androgenic Steroid Abuse on the Cardiovascular System, International Journal of Molecular Sciences, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12652398/
- Systematic review and meta-analysis (35 studies, ~2,000 men): AAS associated with reduced LV ejection fraction and global longitudinal strain, increased wall thickness and LV mass. International Journal of Cardiology, 2026.
- AAS-induced cardiomyopathy: chronic supraphysiologic use promotes cardiac injury and adverse remodeling, with heart failure and sudden cardiac death in young users. Biomedicines, 2025.
- Recovery from anabolic steroid-induced hypogonadism is variable and depends on age and degree of abuse; testosterone, testicular size, and spermatogenesis recover over months to years if at all. Endocrine Connections, 2023.
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents: increase insulin secretion, suppress glucagon, delay gastric emptying, increase satiety. Glucagon-Like Peptide-1 Receptor Agonists, StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide trial: mean weight loss 15.0% to 20.9% across doses versus 3.1% placebo at 72 weeks. New England Journal of Medicine, 2022 (Jastreboff et al.).
- 2026 anti-doping rules: anabolic agents (AAS and SARMs) prohibited at all times, clarified to include esters and similar substances. USADA athlete advisory on the 2026 WADA Prohibited List.
Is any of this actually legit, or is it mostly gym-bro noise?
Both categories are legitimate parts of medicine, but the way they get used in fitness circles is a different story from the clinical record. Anabolic steroids have decades of clinical data behind them, mostly from therapeutic use in hypogonadism and wasting diseases. Peptides like BPC-157 or CJC-1295 have far thinner human trial data by comparison. Legitimate medical use exists for both, but a lot of what circulates online sits in the gray zone research chemicals occupy, not in regulated medicine.
What does this stuff actually cost, and why such a gap in price?
Costs are all over the map depending on where you’re sourcing from. Black-market anabolic steroids can run anywhere from a few dollars a vial to well over a hundred, with purity a total unknown. Peptides bought as research chemicals look cheap upfront but carry similar purity risk. Going through a physician-supervised compounding pharmacy like FormBlends costs more, but you’re paying for verified synthesis, dosing accountability, and an actual prescriber in the loop, which is what that extra cost is buying.
Which one wins for body composition changes?
Anabolic steroids produce faster, more pronounced changes in muscle mass and strength, and the evidence for that is solid. Peptides that target growth hormone release, like sermorelin or ipamorelin, work more gradually and tend to have a milder side-effect profile based on current data. Neither wins universally. It comes down to your goals, your baseline health, and whether you actually have a prescriber willing to monitor you the whole way through.
Where do people actually get this stuff, and what should I know before going that route?
Most people end up on one of three paths: a prescribing physician or anti-aging clinic, a compounding pharmacy, or an unregulated online vendor marketing products as research chemicals. That third path is where the real risk lives. Purity, accurate dosing, and contamination are genuine concerns with unregulated sellers, and there’s no recourse if something goes wrong. The supervised medical route is slower and comes with more paperwork, but it also means a licensed person is actually accountable for what you receive.
Talia Rosenberg is a lay reporter, not a clinician, who spent about a week working through the primary literature and public regulatory records cited above before writing this piece. She has no medical credentials and this piece should not be read as clinical advice.
For general awareness only. Decisions about medication belong with you and your clinician.




